Acute Coronary Syndrome
(Myocardial infarction including NSTE-ACS/NSTEMI and STEMI)
65 y/o M with h/o HTN, CAD, HLD, previous MI, CKD, DM, smoking presents with acute onset chest pain. Reports two episodes of chest and L arm pain similar to previous angina episodes within the past 24 hours. Pain severity acutely increased prior to presentation. Medications include ASA with last use within previous 7 days. Records show coronary artery stenosis ≥ 50%. Family h/o MI-related death 1st degree M relative <55 y/o and 1st degree female relative <65 y/o. Hypotension, diaphoresis, pulmonary crackles, and transient mitral regurgitation on exam. Pain not reproducible with palpation.
≥ 2 indicated need for urgent evaluation
≥ 4 indicates high likelihood of CAD as the cause of chest pain (LR 11.2)
Stat troponins values > 0.150; obtain repeat troponins at 3 and 6 hours s/p initial draw
Stat EKG obtained within 10 minutes of presentation shows NSTE-ACS vs. STEMI (see below for specific treatment)
Treatment
Initial therapy
Aspirin: Chew non-enteric coated 325 mg at symptom onset
Nitroglycerin 0.4 mg sublingually q5 minutes for up to 3 doses as BP allows
SPO2 <90%: Start oxygen 4L by NC
Heparin 60 u/kg IV bolus (max 4,000 u) followed by 12 u/kg/hr infusion (max 1,000 u/hr) to maintain aPTT 1.5-2.0 until revascularization (see STEMI) or 48 h s/p symptom onset
Consider morphine 4-8 mg IV q15 min for refractory chest pain
Treatment based on EKG findings
NSTE-ACS
ST depression in contiguous leads ≥ 0.5 mm, T wave inversion, and new onset Q waves
Able to take aspirin; administer clopidogrel 600 mg loading dose
STEMI: ST elevation and new onset L bundle branch block (see notes for details)
Percutaneous coronary intervention (PCI) capable facility: Complete PCI within 12 hours of symptoms onset and administer clopidogrel 600 mg s/p procedure
PCI not available and pt < 75 y/o with CrCl > 30: Transfer to a capable facility (preferred) or administer clopidogrel 300 mg and fibrinolytic therapy (tPa)
Additional therapy
Start carvedilol 6.25 mg BID and titrate as tolerated
Start lisinopril 2.5 mg qd within 24 hours of symptoms onset; titrate to 10 mg qd
Continue clopidogrel 75 mg qd maintenance therapy x12 months
Start atorvastatin 80 mg qd
Establish outpatient appointment with cardiologist upon discharge
Notes
Epidemiology
CAD risk factors include HTN, HLD, DM, current smoking, and family h/o CAD
Average age at first MI is 65 years
Most predictive s/sx include abnormal stress test, h/o peripheral arterial disease, diaphoresis, acute hypotension, and EKG changes
Myocardial infarction terminology
MI definition: Ischemia-induced cardiac muscle damage resulting in elevated troponins (>3x ULN) and one of the following
Signs or symptoms of ischemia
New, significant EKG changes (see below)
New cardiac wall motion abnormality on echo
Ischemia subtypes
Type 1: Thrombotic occlusion of a vessel
Type 2: Myocardial oxygen demand exceeds oxygen supply
Non-ST elevation myocardial infarction (NSTEMI)
Term no longer used by the American College of Cardiology
Now grouped with unstable angina and known as non-ST elevation acute coronary syndrome (NSTE-ACS)
Troponins >3x ULN are considered significant; this value varies locally and >0.150 is used an example above because it applies to this author’s local institution
EKG changes
ST elevation: Anatomically contiguous lead changes that meet any of the following criteria:
≥ 2 mm in men or ≥ 1.5 mm in women for leads V2-3
≥ 1 mm for leads V1, V4-6, I-III, AVL, AVF
New onset L bundle branch block in the setting of acutely elevated troponins is considered an MI (STEMI) equivalent
Absolute contraindications to fibrinolytic therapy (e.g. tPa)
Blood pressure
Systolic BP > 180 mmHg, diastolic BP > 100 mmHg
R vs. L arm pressure > 15 mmHg
CNS
Closed head trauma within previous 3 months
Any history of intracranial bleeding
Ischemic stroke > 3 hours or within previous 3 months
Structural CNS disease (vascular malformation, neoplasm, etc.)
Pregnancy
ESRD
Metastatic malignancy
Surgery within the past 4 weeks

Right Bundle Branch Block with STEMI due to LAD occlusion. Photo credit Dr. Stephen W. Smith .

12 Lead ECG EKG showing ST Elevation (STEMI), Tachycardia, Anterior Fascicular Block, Anterior Infarct, Heart Attack. Color Key: ST Elevation in anterior leads=Orange, ST Depression in inferior leads=Blue
Thrombolysis in MI Risk Score
1 point for each:
Age>64
3+ CAD risk factors
Known CAD with >50% stenosis
Aspirin use within past 7 days
2+ anginal episodes within preceding 24 hours
Elevated troponin I
ST segment deviation >0.5mm on admission ECG
Interpretation
Low risk (0-2): Stress test
Intermediate (3-4) to high (5-7) risk: Coronary angiography within 24 hours
Immediate coronary angiography for hemodynamic instability, heart failure/new MR, recurrent chest pain, ventricular arrhythmia
Atrial Fibrillation with Rapid Ventricular Response
Elderly pt with h/o psychosis, depression presents s/p cardiac surgery with palpitations and s/sx suspicious for HF vs. MI vs. stroke. Reports fatigue, chest pain, syncope, dizziness, dyspnea, and orthopnea. Medical history includes coronary artery disease, structural heart disease, heart failure, collagen vascular disease, pulmonary disease, sleep apnea, thyroid disease, and ongoing substance abuse. Medications include OTC diet pills, albuterol, lithium, and QTc-prolonging agents. Hypothermia, tachycardia, JVD, pulmonary crackles, systolic heart murmur, S3 gallop, irregular peripheral pulses on exam.

Atrial fibrillation with Rapid Ventricular Response (RVR)
Labs
Obtain CBC, CMP, TSH
Consider urine drug screen
EKG: Rapid, irregularly irregular rate with absent P-waves, narrow Q-waves
New onset with no previous echocardiogram: Obtain echocardiogram to evaluate for valvular A-Fib
Rate control
Patient stable: Maintenance rate control with goal HR < 110 bpm at rest
SBP > 100 mmHg: Metoprolol tartrate 25 mg BID (MDD 100 mg BID)
SBP < 100 mmHg: Digoxin 0.125 mg daily (MDD 0.25 mg daily)
Acute hypotension, altered mental status, chest discomfort or HR consistently > 120 BPM:
SBP > 100 mmHg: Cardizem 0.25 mg/kg bolus over 2.5 min then 10 mg/hr infusion for up to 24 hr
SBP < 100 mmHg and/or HFrEF: Digoxin 0.25 mg; re-dose q6h to achieve HR < 110 bpm
Rate control ineffective
Obtain cardiac consult
Consider cardioversion if AFib duration < 48h or pt hemodynamically unstable
Stroke prevention
CHADSVASC > 1, HASBLED < 3, age > 80 years, weight > 60 kg, Cr < 1.5, and no valvular AFib on echocardiogram: Start abixaban (Eliquis) 5mg BID
Consider referral for
Cardiac and/or left atrial appendage ablation
Watchman device placement
Pacemaker placement
Refer for sleep apnea testing as outpatient
Counseling
Pt counseled that spontaneous A-Fib generally resolves within 7 days
Pt advised to limit alcohol consumption to < 1 drink per day
Notes
Considerations
Increase A-Fib risk
Commonly associated agents include anti-arrhythmics, antidepressants, anti-psychotics, fluoroquinolones, macrolides, and antifungals
Heart rate
A-Fib is a tachycardia with HR generally between 90-170 BPM; consider sick sinus syndrome in bradycardic patients
A-Fib with RVR (rapid ventricular response) rarely causes clinical instability unless HR > 150 bpm
Rate control
Rate control equivalent to rhythm control per AFFIRM trial (N Eng J Med. 2002;347(23):1825-1833)
Lenient control (HR < 110) per RACE II trial (N Eng J Med. 2010;362(15):1363-1373)
Rate control advanced organizers:
ABCD: A-Fib agents include Beta-blockers, Cardizem, Digoxin
Maintenance agents: Beta-blocker (metoprolol) or digoxin
Acute agents: Cardizem or digoxin
Rule of '0.25' for acute dosing, i.e. Cardizem 0.25 mg/kg bolus over 2.5 min or digoxin 0.25 mg
Metoprolol succinate
Long acting oral formulation
Provide most effective heart rate control at rest and during exercise
Contraindications: Systolic pressure <100 mmHg, h/o Wolff-Parkinson-White syndrome
Diltiazem (Cardizem): Often used off-label for maintenance dosing
Initial dose: Immediate release 60 mg BID
Maximum dose 120mg TID
Contraindication: Systolic <100 mmHg
Digoxin: Used off-label for maintenance dosing in patients with hypotension
Rhythm control
For stable patients with A-Fib duration >48h, one of the following is required before cardioversion:
Anti-coagulation for 4 weeks
TEE to rule out presence of atrial thrombus
Unstable patients
Amiodarone IV: 150 mg over 10 minutes, then 1 mg/minute x6 hours, then 0.5 mg/minute x18 hours, then oral maintenance dosing
Synchronized electrical cardioversion: 120-200J biphasic or 200 J monophasic
Stroke
Stroke risk
5 times greater in patients with AFib
Further elevated if AFib is caused by valvular disease
Valvular disease includes mechanical heart valves, rheumatic heart disease/mitral stenosis, decompensated heart failure due to valve dysfunction
Use warfarin (Coumadin) to anticoagulate these patients
Stroke prevention
CHADSVASC: Aspirin if equal to 1, anticoagulation for score of 2 or greater
HASBLED determines bleeding risk; score of 3 or greater indicates high risk
Apixaban (Eliquis)
May not be covered by insurance
Not approved for use in pregnancy, dialysis, or valvular A-Fib
Watchman device occludes LA appendage and reduces embolization risk
CHADS-VASc
Used to calculate stroke risk in patients with atrial fibrillation.
CHF: +1
HTN: +1
Age: 65-74 [+1], >75 [+2]
DM: +1
Stroke: +2
Vascular disease: +1
Sex F: +1
1 point for each of the following:
Hypertension >160mmHg systolic
Abnormal renal function, i.e.
Dialysis
Transplant
Cr >2.26 mg/dL or >200 µmol/L
Abnormal liver function, i.e.
Cirrhosis
Bilirubin >2x normal + AST, ALT, or AP >3x normal
Stroke: Prior history of stroke
Bleeding: Prior Major Bleeding or Predisposition to Bleeding
Labile INR, i.e.
Elevated INR
INR within therapeutic Range < 60% of the time
Elderly: Age > 65 years
Drugs: Antiplatelet agents, NSAIDs, ≥ 8 drinks/week"
Additional Arrhythmias
AV Block
First degree
Second degree
Mobitz 1 → Treat underlying condition, e.g.
Ischemia affecting AV node
Hypothyroidism
Mobitz 2 → Pacemaker
Third degree heart block → Pacemaker
Sinus Node Disease (Sick Sinus Syndrome)
Risk factors: Age > 60 years, CAD, hypothyroidism, medications
May present with persistent tachycardia, persistent bradycardia, or tachy-brady syndrome
Symptomatic patients: Refer for pacemaker placement
Torsades de Pointes
Polymorphic ventricular tachycardia
Risk factor: Electrolyte imbalance (e.g. hypokalemia), medications
Often progresses to ventricular fibrillation
Treat with magnesium
Heart Failure
Elderly patient with history of hypertension, coronary artery disease, valvular heart disease, atrial fibrillation, and diabetes mellitus type 2 presents with dyspnea on exertion, fatigue. Reports new onset orthopnea, nocturnal cough. Heart rate > 120 bpm, jugular venous distention, hepatojugular reflux, bibasilar crackles, S3 gallop, 2+ pitting lower extremity edema on exam.
Patient meets Framingham heart failure diagnostic criteria
Labs
NTpBNP > 400 pg/mL
Obtain CBC, ferritin, TIBC, CMP
Consider lipid profile, TSH, U/A, HbA1c
Imaging
Atrial fibrillation on EKG
CXR shows cardiomegaly, venous congestion, interstitial edema with Kerley B lines
Echocardiogram shows (one of the following patterns):
Preserved ejection fraction: LVEF > 50%, elevated LA pressure, impaired LV relaxation, decreased compliance, and E/A reversal
Reduced ejection: LVEF < 50%
Treatment
Patient counseled about weight loss, dietary sodium reduction, smoking cessation
ACE inhibitor: Lisinopril
Preserved ejection fraction: Start 5 mg daily and increase by 10 mg every two weeks to target dose of 40 mg daily
Reduced ejection fraction: Start 10 mg daily and titrate to 20 mg daily as needed for blood pressure control
Additional medications
EF < 40%: Metoprolol succinate 50 mg daily
Symptomatic (e.g. dyspnea): Chlorthalidone 25 mg daily
Start statin if patient qualifies
Atrial fibrillation at any EF
Aspirin 81 mg + anticoagulation per CHA2DS2-VAsc
Metoprolol succinate 50 mg daily
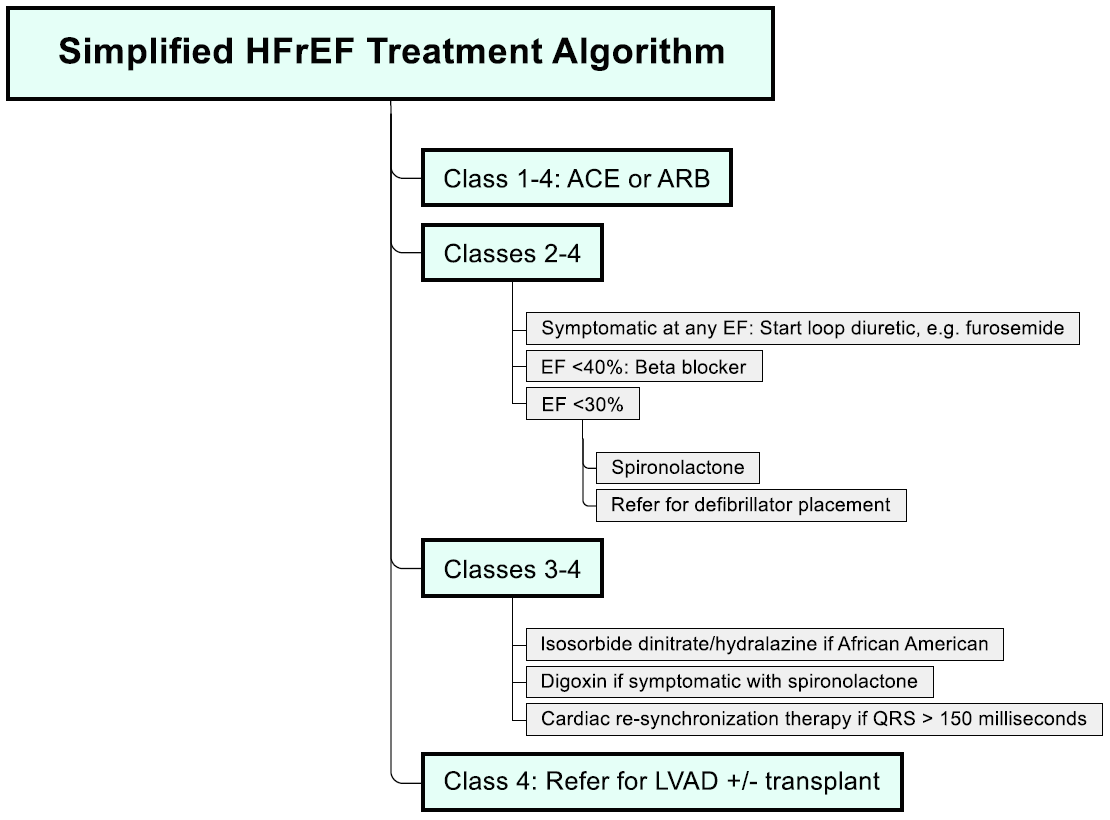
Heart failure with reduced ejection fraction (HFrEF)
Hypervolemia
Fluid restrict to 1.5 L daily to correct hypervolemia, hyponatremia
Hypervolemia refractory to fluid restriction: Stop chlorthalidone, start bumetanide 1 mg daily and titrate to 2 mg daily
Ferritin < 100 ng/mol
Administer 1000 mg IV iron ferric carboxymaltose bolus
Schedule follow-up at 6, 12, 24, and 36 weeks to monitor anemia
LVEF < 30% with GFR > 30 mL/min
Start spironolactone 12.5 mg daily and double dose every 4 weeks to 50 mg daily while monitoring for hyperkalemia
Persistent symptoms despite spironolactone: Consider digoxin 0.125 mg daily
LVEF < 30% and fatigue, palpitation, dyspnea, or anginal pain provoked by moderate exertion: Consult cardiology for defibrillator placement
Additional considerations
Consider transition of ACE to Entresto (valsartan + sacubitril) in patients with HFrEF class II-III to improve outcomes
African American with uncontrolled HTN on ACE/beta-blocker: Consider isosorbide dinitrate/hydralazine (Bidil) 1 tablet TID
Angina/chest pain present: Obtain stress test (may require catheterization)
Follow up as outpatient within 7 days after hospital discharge to reduce readmission rate
Notes
Non-hypertensive Causes of Heart Failure
Cardiac: Pericardial constriction, primary valvular disease, atrial myxoma
Infiltrative disorders: Amyloidosis, sarcoidosis
Storage disorders: Hemochromatosis
NYHA Stages of Heart Failure
No limitation of physical activity
Light limitation of physical activity: Ordinary activity causes fatigue, palpitations, or dyspnea
Marked limitation: Less than ordinary activity causes fatigue, palpitations, or dyspnea
Unable to engage in physical activity without symptoms, or symptoms that occur at rest
HFpEF
Definition: EF > 50% with s/sx of HF (diagnosis of exclusion)
Pathophysiology
Reduced ventricular compliance reduces ventricular filling during diastole
Most commonly associated with LV hypertrophy
Treatment
Controlling hypertension improves prognosis
Beta-blockers reduce heart rate and improve ventricular filling
HFrEF
Medications that improve mortality
Beta-blockers
Approved agents: Metoprolol succinate, carvedilol (Coreg), bisoprolol
Start in all patients when euvolemic and stable
Contraindications: Hemodynamic instability, bradycardia, severe asthma
Aldosterone antagonists (e.g. eplerenone, spironolactone) in patients with EF < 35% and symptomatic HF (survival advantage observed within 30 days)
Vasodilators: Hydralazine, isosorbide dinitrate
Additional medications
Diuretics and digoxin: Improve symptoms, but do not decrease mortality
Amlodipine may help control blood pressure, but does affect HF outcomes
Verapamil: Negative inotropic effect worsens heart failure
Statins do not improve outcomes for patients who do not otherwise meet criteria for lipid-lowering therapy, see CORONA, GISSI-HF trials
BNP
Volume expansion → increased ventricular pressure → ventricular dysfunction → BNP release
Renally cleared, i.e. ↓ Cr clearance = ↑ BNP
BNP > 400
LR = 19 for heart failure
Does not necessarily indicate acute exacerbation
HF exacerbation: BNP at admission is correlated with inpatient mortality
Dilated Cardiomyopathy
45 y/o pt with h/o autoimmune disease, DM, Hep C, HIV, alcoholism, malignancy s/p radiation/chemotherapy presents with SOB. Pt has noted new onset palpitations and was recently treated for DVT. Reports family h/o dilated cardiomyopathy. Tachycardia, lower extremity edema on exam.
Obtain CMP
EKG shows T wave changes, septal Q waves, bundle branch block
Echo shows ventricular enlargement with normal left ventricular wall thickness and reduced ejection fraction
Reduced ejection fraction: Start lisinopril 5 mg qd, metoprolol succinate 25mg qd
NYHA class 2 or greater with reduced ejection fraction and GFR>30: Start Entresto (sacubitril/valsartan) 24/26 mg s/p 36 hour washout period for previous ACE
Notes
Approximately 30% of cases are familial
ACEs/ARBs provide significant mortality benefit in patients with reduced ejection fraction
Hypertrophic Cardiomyopathy
Pt with h/o dyspnea on exertion presents with recurrent, acute chest pain. Chest pain generally occurs during meals or exercise and is more common during summer months. Family h/o sudden, unexplained cardiac death. Systolic murmur with increased intensity during Valsalva on exam.
EKG shows left ventricular hypertrophy (LVH), Q-waves
Echocardiogram shows LVH with decreased chamber volume
LVEF < 50%
Refer to heart failure (HFrEF) treatment guidelines
Plus anginal symptoms: Start nadolol 40 mg qd
Refer for implantable cardioverter-defibrillator (ICD) placement for any of the following:
H/o sudden death in 1st degree relative
Ventricular wall thickness > 30mm
Sustained ventricular tachycardia and/or cardiac arrest
Pt counseled that alcohol septal ablation or surgical myomectomy may be necessary for end-stage heart failure
Notes
Prevalence 1:500
Chest pain worse with dehydration
Valsalva reduces preload/filling, resulting in less blood in the heart
Takotsubo Cardiomyopathy
Postmenopausal female presents with acute-onset chest pain. Reports recent dyspnea, syncope, emotional/physiologic stressors. No h/o myocarditis, pheochromocytoma, cocaine use. Tachycardia, hypotension, respiratory distress, cold extremities on exam.
Labs
Initial troponin >0.02
Obtain troponin x3, pro-BNP; consider UDS to r/o cocaine use
Strict I&O's; monitor for oliguria
Imaging
EKG shows ST-segment elevation and/or T wave inversion
Echocardiogram shows LV dysfunction and LV apical ballooning; no evidence of obstructive coronary disease
Angiography shows no evidence of acute plaque rupture
Treatment
Manage acute cardiogenic shock per ACS guidelines
Once stable, start lisinopril 10 mg daily, metoprolol succinate 25 mg daily, HCTZ 25 mg daily
Loss of LV wall motion on echocardiogram: Start abixaban 5mg BID x4 months for thrombus ppx
Pt counseled that symptoms typically resolve within 1 month
Notes
Prevalence
Affects 1 in every 5,000 hospitalized patients
Responsible for 1 in every 75 cases of troponin-positive ACS
Aortic Dissection and Aneurysm
Aortic Dissection
65 y/o M with h/o HTN present with acute back pain. Pain is inter-scapular and tearing in nature. Reports syncopal episode s/p pain onset. Asymmetric blood pressure and upper extremity pulses on exam.
CT with contrast shows dissection
Contraindication to IV contrast: Obtain transthoracic (TTE) and/or transesophageal echo
Treatment
Start IV esmolol to reduce LV ejection velocity
Start IV nitroprusside to lower systolic blood pressure to 90-110 mmHg
Note: Syncope occurs in 9% of patients with aortic dissection
Abdominal Aortic Aneurysm (AAA) Screening
Etiology and Epidemiology
Due to atherosclerosis
Affects 2-5% of patients > 65
Approximately 5:1 male:female predominance
USPSTF recommends one-time screening for AAA with ultrasound in men ages 65-75 who have ever smoked (i.e. >100 cigarettes in a lifetime)
Management based on diameter:
AAA < 5.5 cm in men: Repair for growth > 0.5 cm in 6 months or > 1 cm per year
Aneurysm 3.0 to 4.0 cm: Ultrasound yearly
Aneurysm 4.0 to 5.5 cm: Ultrasound every 6 months for one year and then yearly if no growth
AAA > 5.5 cm in men or > 5.0 cm in women:
Life expectancy > 2 years and a surgical candidate: Refer for surgical endovascular repair
Life expectancy < 2 years: Do not repair
Abdominal Aortic Aneurysm Rupture
65 y/o M with a h/o HTN, AAA, and Marfan’s syndrome presents with acute onset abdominal pain radiating to the flank and groin. Reports associated vomiting and syncope. Hypotension on exam with a pulsatile abdominal mass.
STAT non-contrast abdominal CT shows AAA rupture
Obtain STAT vascular surgery consult
Patient’s family counseled that condition is associated with 80% mortality rate
Peripheral Arterial Disease
Pt age > 65 years h/o HTN, HLD, CVA, heart failure, chronic kidney disease, DM, smoking presents with calf pain/cramping during activity. Pain resolves after approximately 10 minutes rest. Diminished pulses, pallor, hair loss, and non-healing gangrenous wound on lower extremities; ankle-brachial index 1.3 < ABI < 0.9.

Acute limb ischemia due to arterial thrombosis. James Heilman, MD - Own work.
Obtain CBC, CMP, BNP
Lipid panel shows HDL < 50 mg/dL
EKG shows Q waves and ST segment changes
Treatment
Start supervised exercise therapy program
Start aspirin 81 mg qd, ramipril 2.5 mg qd x 1 week and then 5 mg qd, atorvastatin 80 mg qd
Continued pain s/p supervised exercise therapy and no h/o heart failure: Start cilostazol 100 mb BID; pt counseled about risk for dizziness, GI distress due to vasodilatory effects
Consults/Referral
Refer for surgical revascularization for cases of
Lifestyle limiting claudication with insufficient response to exercise/medical therapy
Ischemic rest pain x 2 weeks
Admit to hospital for emergent vascular surgery within 4 to 6 hours in cases of limb-threatening ischemia as indicated by painful, pale/dusky colored and cold extremity with absent pulses, motor weakness, sensory impairment
Pt advised to stop smoking and offered smoking cessation therapy
Notes

5 MHz vascular Doppler probe used for ABI

2 MHz fetal Doppler probe used for prenatal care after 14 WGA
Epidemiology
Affects 50% of patients age > 85
Only 10% of PAD patients experience claudication
Diagnosis
Ischemic rest pain generally occurs when feet are elevated and resolves in the dependent position, e.g. sleeping pt must hang feet over side of bed
Ankle-brachial index (5-8 MHz vascular probe not 2-3 MHz fetal probe)
94-97% sensitivity for detecting angiographically significant stenosis
Values > 1.3 suggest non-compressibility; use toe index with > 0.7 considered normal
HDL < 40 and 50 mg/dL in males/females receptively is associated with increased risk of death
Consider BNP to r/o heart failure before starting cilostazol
Treatment
Dual antiplatelet therapy is generally not more effective than aspirin
Heart Outcomes Prevention Study: ACE (ramipril) or ARB (telmisartan) reduced MI, stroke, and mortality in patients with PAD and no h/o heart failure
Statin NNT ~ 5 to reduce risk of long-term adverse outcome
Supervised exercise therapy can often be performed at a physical therapy center; otherwise, pt should walk until pain onset and then rest until pain subsides
Cilostazol contraindicated in heart failure
Undifferentiated shock
Pt with h/o respiratory compromise, arterial occlusion presents with acute onset hemodynamic instability. Tachycardia, tachypnea, hypotension, confusion/delirium, increased WOB, dry mucous membranes, JVD, arrhythmia, cyanosis/mottling on exam. Systolic BP <90 with MAP <65; urine output <0.5 mL/kg/hr.
Labs
Obtain CBC with diff, CMP, ABG, serum lactate
Obtain troponin, CKMB, BNP, creatinine kinase
Obtain U/A, blood cultures, sputum cultures
Obtain type and PT/PTT/INR, D-dimer
Consider urine drug screen
Triage
ABG shows high anion gap metabolic acidosis, serum lactate >2
Serum lactic acid >4: Transfer pt to MICU
Imaging
Obtain EKG, CXR, U/S of IVC
Start continuous cardiac telemetry
CT if concern for trauma and/or intracranial hemorrhage
Stabilize respiratory status
Titrate supplemental O2 to maintain SPO2 > 92%: Administer oxygen via NC 6L/min; if insufficient proceed to HFNC 20L/min, then BiPAP 12/5, and finally intubation
GCS<8 or marked respiratory distress/hemodynamic instability with no suspected tension pneumothorax: Administer ketamine 1.5 mg/kg IV, rocuronium 1.5 mg/kg IV and intubate
Specific interventions
Anaphylaxis: IV epinephrine
Tension pneumothorax: Chest tube
Massive pulmonary embolus: Thrombolytic therapy
Circulatory
Establish IV access; administer 1L LR bolus followed by maintenance fluid
If peripheral access cannot be obtained and/or vasopressors indicated, place central line
MAP <65 s/p fluid resuscitation; start noradrenaline (Levophed) at 0.2 mcg/kg/hr and titrate to MAP >65
Specific interventions
Stroke: Evaluate for tPA; consult neurology
Arrhythmia with hemodynamic decompensation: ACLS protocols
Myocardial infarction: Coronary revascularization
Cardiac tamponade: Pericardiocentesis
Sepsis
Initiate broad-spectrum antibiotics
Calculate Q-SOFA score
Notes
MAP > 60 required to maintain cerebral perfusion
Serum lactate
>2 indicates likely shock
>4 is "not for the floor" as it predicts increased mortality independent of organ hypoperfusion
Q-SOFA score
One point for each of the following
GCS <15
Respiratory rate >21
SBP <101
Score of 2 or greater indicates high risk of poor outcome in patients with suspected infection, i.e. 3 to 14 times higher risk of in-hospital mortality
Cardiogenic shock
Pt with h/o severe HTN, DM, CAD, MI, HFrEF, dilated cardiomyopathy, aortic stenosis, stable abdominal aortic aneurysm presents with arrythmia s/p ingestion of beta-blockers during suicide attempt. Reports dyspnea, acute on chronic chest pain, syncope, recent chest trauma, and alcohol/cocaine abuse. Systolic BP < 90 mmHg, bradycardia, tachypnea, JVD, bibasilar pulmonary crackles, mid-systolic ejection murmur at R upper sternal border, cool extremities, confusion on exam.
Obtain CBC, CMP, serial troponin, ABG, lactic acid, PT/PTT/INR
Obtain EtOH level, urine drug screen
Strict I&O’s and monitoring for oliguria
EKG shows myocardial ischemia: Evaluate for acute coronary syndrome
CXR shows tension pneumothorax and new onset pulmonary congestion
CTA shows pulmonary embolism
Obtain echocardiography; evaluated for acute myopericarditis, takotsubo cardiomyopathy, HFrEF, pericardial tamponade, ascending aortic dissection
Treatment based on underlying condition
Notes
May be due to the heart itself (vessel/muscle/valve), arrhythmia (tachy/brady), or obstruction
Heart defects
Vessel infarction → ischemia → acute coronary syndrome
Muscle
Dilated cardiomyopathy (consider in pt with h/o alcohol abuse)
Acute myopericarditis
Cardiac contusion
Valvular insufficiency: Severe valvular stenosis, chordae tendinae rupture, valvular stenosis, ventricular septal wall defect/rupture
Arrhythmia: Treat per ACLS guidelines
Obstruction
Decreased cardiac return
Vena cava syndrome
Massive pulmonary embolism
Cardiac compression
Tension pneumothorax
Pericardial tamponade
Outflow obstruction: Ascending aortic aneurysm
Distributive shock
Pt with h/o anaphylactic shock, hypothyroidism, hypoadrenalism presents with spinal trauma. Recently diagnosed with group A strep pneumonia and suffered bee sting prior to admission. Fever, hypotension, confusion/delirium, facial edema, dry mucous membranes, inspiratory stridor, hives, skin warmth below level of spinal injury, localized area of skin necrosis with abscess on exam. No LE edema, JVD noted. Systolic BP < 90 with MAP < 65, urine output < 0.5 mL/kg/hr.
Diagnostic approach
Obtain q 1 hour vital signs until stable
Obtain CBC with differential, CMP, ABG, type and cross
Obtain serum lactate now, at 2 hours, and then q6h until stable
Obtain blood culture, sputum culture, U/A with culture, wound culture
Obtain troponin, CKMB, BNP, creatinine kinase
U/S shows IVC > 1.5 cm, i.e. adequate blood volume
Initial treatment
Secure airway, correct hypoxemia (nasal cannula → high flow nasal cannula → BiPap)
Transfuse for hemoglobin < 7 g/dL
Place central line if peripheral access cannot be obtained and/or vasopressors indicated
Administer 1L LR bolus followed by maintenance fluid (goal = 30 mL/kg over 3 hours) before starting vasopressors
MAP < 65 s/p fluid resuscitation: Start noradrenaline (Levophed) at 0.2 mcg/kg/hr and titrate to MAP > 65
Anaphylactic shock
Administer 0.3 mg epinephrine 1:1000 injected in outer thigh q 10 min
Administer diphenhydramine 50 mg IV, ranitidine 50 mg IV, methylprednisolone 1 mg/kg IV
Administer albuterol 2.5 mg nebulized solution
Septic shock
Initial CBC shows bandemia
Obtain blood culture from two distinct venipuncture site and any indwelling devices
Start linezolid (Zyvox) IV 600 mg BID, Zosyn 3.375 g IV q8h
Suspected infection source
CNS (e.g. meningitis): CSF cell count, protein, glucose, Gram stain, and culture
Respiratory tract: Start chest physiotherapy, suctioning for pneumonia
Intra-abdominal: Obtain abdominal CT +/- stool culture
Urinary tract: Change catheter and consult urology if urinary tract obstruction suspected
Skin and soft tissue: Debride necrotic tissue, drain abscess and/or effusion
Bone: Obtain MRI +/- bone culture
Indwelling device: Discontinue or replace access site
Myxedema coma/adrenal crisis
Obtain TSH, free T4 serum cortisol, ACTH, aldosterone, renin
Administer levothyroxine 300 mcg IV, followed by 75 mcg qd
Administer triiodothyronine 10 mcg intravenously, followed by 5 mcg q8h
Administer hydrocortisone 100 mg IV q8h until adrenal insufficiency excluded
Consult endocrine
Neurogenic shock
Obtain CT at level of traumatic spinal cord injury (TSCI)
Presenting within 8 hours of isolated, non-penetrating TSCI: Consider methylprednisolone 30 mg/kg IV bolus followed by 5.4 mg/kg infusion x 23 hours
Consult neurology
Notes
Potential distributive shock etiologies
Infectious
Septic shock (e.g. pneumonia)
Group A streptococcal infection (e.g. skin necrosis)
Non-infectious
Anaphylactic shock (characterized by allergen exposure followed by facial edema, inspiratory stridor, hives)
Endocrine etiologies including adrenal crisis, myxedema coma due to hypothyroidism
Neurogenic shock
Antibiotics: Zyvox, Zosyn, aZithromycin for pan coverage
Linezolid: Gram positive coverage including MRSA (neurotoxicity risk limits use to < 2 weeks)
Zosyn
Covers anaerobes and gram negative organisms including pseudomonas
Does NOT cover Legionella
Does NOT cover organisms with inducible beta-lactamase activity that is chromosomally mediated, i.e. ESCHAPPM (Enterobacter, Serratia, Citrobacter freundii, Hafnia, Aeromonas, Proteus vulgaris, Providencia, Morgananii)
Azithromycin: Covers Legionella
Moxifloxacin: Covers Legionella and ESCHAPPM organisms
Antifungal: Mycofungin 100mg IV qd if disseminated fungal infection is present
Hypovolemic shock
Pt with h/o pancreatitis, intestinal obstruction, polyuria presents with blood loss s/p crush injury. Reports N/V, diarrhea s/p completing a marathon. Orthostatic hypotension, tachycardia, acute weight loss, dry mucous membranes, bleeding cool/mottled extremities, delayed capillary refill, weakness, crush injury, and agitation/confusion on exam.
Obtain CBC, CMP, serial troponin, ABG, lactic acid, PT/PTT/INR
Obtain urine sodium, creatinine, osmolality
Urine sodium <20 mEq/L, FENA <0.2, urine osmolality >450 mOsmol/kg
Strict I&O’s; monitor for oliguria
Bedside U/S shows IVC diameter <1.5cm
Establish access using two large-bore IVs
Administer 2L LR bolus; give additional boluses until MAP>65
Massive blood loss, hemoglobin <7: Adminster PRBCs
Notes
Third-spacing may occur due to intestinal obstruction, crush injury, fracture, and acute pancreatitis
Low urine sodium and elevated urine osmolality strongly suggest tissue hypoperfusion; exceptions include
Patients with polyuria due to hypoaldosteronism, diuretic abuse, etc.
Metabolic alkalosis due to vomiting
FENA = ([Plasma creatinine × urinary sodium] / [plasma sodium × urinary creatinine]) × 100
Do NOT administer vasopressors